Duchenne muscular dystrophy: dangerous hereditary muscular dystrophy
Muscular dystrophy is a group of diseases that cause muscle atrophy and weakness. Of these, Duchenne muscular dystrophy is the most common. This is a disease that progresses gradually over time and seriously affects health. Early recognition and appropriate treatment prolong survival. The following article will explain more about this disease.
content
- 1. What is Duchenne muscular dystrophy?
- 2. What is the cause of Duchenne muscular dystrophy?
- 3. Symptoms and signs of Duchenne muscular dystrophy
- 4. How is Duchenne muscular dystrophy diagnosed?
- 5. How is Duchenne muscular dystrophy treated?
- 6. Genetic counseling and disease monitoring?
1. What is Duchenne muscular dystrophy?
Duchenne muscular dystrophy (DMD) is an inherited disease. This pathology is characterized by progressive, irreversible muscle atrophy. This condition does not affect only the musculoskeletal system. In the late stages, it can act on cardiac and smooth muscle.
Duchenne muscular dystrophy is a recessive genetic disease on the X chromosome. Therefore, it is common in boys, with an incidence of 1/3500. However, a small percentage of the disease occurs in girls. And in some cases, the gene for the disease was not found on the mother's X chromosome.
2. What is the cause of Duchenne muscular dystrophy?
In the human body, each gene is responsible for the production of a different protein. The dystrophin gene is located on the X sex chromosome at Xp21.2, and is 2400kb long (the longest in humans). It consists of 79 exons responsible for the synthesis of the protein Dystrophin. The dystrophin protein is important for maintaining the structure and function of muscle cells. Dystrophin acts as a "shock absorber". It allows the muscles to contract and relax without injury. Without dystrophin, muscles cannot function or repair themselves.
Sometimes muscle membranes are vulnerable to normal daily activities. Lesions produce microscopic tears in cell membranes. These small tears allow calcium to enter the cells, which is toxic to the muscles. Calcium damages and eventually kills muscle cells. And then they are replaced by scar tissue and fat cells. The loss of muscle then leads to a loss of strength and function.

The mutations that can occur on the Dystrophin gene are deletion mutations, point mutations, and translocations. Small segment deletions and deletions are the most common mutations. Thousands of different mutations have been reported in the dystrophin gene. It is important to remember that no one causes genetic mutations and they cannot be prevented. Each of us carries mutations in some of our genes. Although we often don't know it.
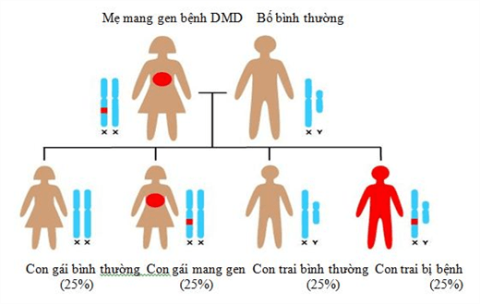
Duchenne disease is caused by a recessive gene mutation. So if a mother carries the disease gene and gives birth to a boy, there is a 50% chance of having the disease. If it's a girl, then 50% of them carry the disease gene but don't show symptoms.
3. Symptoms and signs of Duchenne muscular dystrophy
3.1 The first years of life
DMD often presents early in childhood. Initial symptoms may appear between 2 and 3 years of age. Children with the disease often have weakness and atrophy of the muscles near the trunk (proximal muscles) anteriorly. For example, the muscles of the thighs, groin, arms and shoulders. However, as the disease progresses, weakness and muscle atrophy will spread. It affects the muscles of the legs, forearms, neck, and trunk. The rate of progression is pretty much the same for each person, but differences can occur.
In children with DMD, early findings may include delays in achieving normal developmental milestones. For example, sitting or standing without assistance. In addition, there may be symptoms such as toe walking; abnormal gait with wide base, slightly arched posture; Trendelenburg gait in both legs; difficulty climbing stairs or getting up from a sitting position (Gower sign); and fell many times. Toddlers and young children can appear awkward and clumsy. There may be abnormal enlargement of the calf muscles due to muscle scarring (pseudohypertrophy).
3.2 From 5 to 9 years old
Parents may be secretly delighted by the obvious improvement between the ages of 3 and 5. But this may be due to natural growth and development. As the disease progresses, other abnormalities may appear. Specifically, scoliosis, atrophy of the pectoral muscles, and abnormal contractures of some joints. Contraction occurs when tissues thicken and shorten like muscle fibers causing deformation. This limits movement of the affected areas, especially the joints. Without physical therapy, a leg brace may be needed at ages 8-9 to assist the child in walking.

3.3 Entering adolescence
Between the ages of 10 and 12, most people with the disease need a wheelchair for mobility.
Children with DMD have reduced bone density and an increased risk of breaking some bones. Such as the hip and spine. Many affected people will present with mild to moderate intellectual impairment and learning disabilities.
By late adolescence, DMD can have life-threatening complications. These include weakening and degeneration of the heart muscle (cardiomyopathy). Cardiomyopathy can lead to impaired pumping ability of the heart, irregular heartbeat (arrhythmia), and heart failure. Another serious complication associated with DMD is impaired and reduced respiratory function. Respiratory failure and pulmonary complications are caused by weakness of the diaphragm, intercostal muscles, and other accessory muscles of respiration, which severely reduces the ability of the lungs to ventilate. Weakness of the exhalation muscles, especially the abdominal muscles, also reduces the effectiveness of coughing. Leads to stasis pneumonia, atelectasis.
The muscles in the digestive tract can also become dysfunctional. Food moves through the digestive tract slows down and the muscles don't work together. Gastrointestinal dysfunction may include constipation and diarrhea.
One-third of patients with DMD may have some degree of cognitive impairment. These include learning disabilities, impaired attention, and autism spectrum disorders.

4. How is Duchenne muscular dystrophy diagnosed?
DMD is diagnosed based on a thorough physical examination, taking a detailed patient history, and performing a variety of specialized tests including molecular genetic testing (PCR). If genetic tests are not informative, a biopsy of the affected muscle tissue may show characteristic changes in the muscle fibers.
4.1 Molecular genetic tests
- involves testing for deoxyribonucleic acid (DNA) to identify a specific genetic mutation including deletion, duplication, or single point mutation. Blood or muscle cell samples may be tested. These techniques can also be used to diagnose DMD before birth.
4.2 Blood tests
- may show elevated levels of creatine kinase (CK). An enzyme found at abnormally high levels when muscle is damaged. Detecting elevated CK levels (usually in the thousands or thousands) can confirm muscle damage or inflammation, but cannot confirm a diagnosis of DMD.
- In some cases, a specialized test may be performed on muscle biopsy samples that can determine the presence and levels of specific proteins in the cells. Various techniques such as immunostaining, immunofluorescence or Western blot can be used. These tests involve the use of certain antibodies that react with certain proteins such as dystrophin. Tissue samples from muscle biopsies are exposed to these antibodies. The results can determine if a particular muscle protein is present in the cell and in what amount or size.
- Electromyography: contributes to the diagnosis but has no definite diagnostic value.
- Pulmonary function measurement: measure the degree of ventilation restriction due to respiratory muscle weakness, or chest deformity.
- Electrocardiography and echocardiography to detect and monitor dilated cardiomyopathy.
5. How is Duchenne muscular dystrophy treated?
There is no cure for DMD. Treatments are aimed at the specific symptoms of each individual patient. Access a rehabilitation program that includes physical therapy, active and passive range of motion exercises… to maintain muscle strength and prevent contractures. Surgery may be recommended in some patients to treat symptoms of scoliosis or curvature of the spine. Splints can be used to stop the progression of contracture. The use of mechanical aids (eg, canes, splints, and wheelchairs) may become necessary to assist with walking.
Corticosteroids are used as a standard of care for the treatment of DMD. This drug slows the progression of muscle weakness in affected individuals and delays loss of mobility for 2-3 years.
6. Genetic counseling and disease monitoring?
If there is a family history of Duchenne muscular dystrophy, genetic screening may be useful for early diagnosis and early treatment. These genetic tests can be done on adults, children, and even fetuses in the womb. Once Duchenne muscular dystrophy has been diagnosed, early treatment can help relieve symptoms and slow disease progression.
Once infected, symptoms worsen over time. Families need to be psychologically and fully prepared to face and monitor their child's care properly. Maintaining learning and independently performing daily living activities helps children become more confident in life.
Because Duchenne muscular dystrophy can cause cardiovascular problems, it is very important that children have a cardiovascular exam at least every 2 years until age 10 and then once a year. Girls and women carrying the gene also have a higher risk of heart problems than the general population. They should see a cardiologist in their late teens or early adulthood to check for problems.
Duchenne muscular dystrophy is a progressive disease that progresses to death at a relatively young age with no cure. Thanks to medical advances in recent years, it has contributed significantly to prolonging life. Currently, the role of rehabilitation plays an increasingly important role in improving the quality of life for patients.
Doctor Luong Sy Bac